NATIONAL IMMUNISATION DAYS IN BAMENDA HEALTH DISTRICT, CAMEROON, 1996 – May 2005
INTRODUCTION
National immunisation days (NIDs) constitute supplementary vaccination activities carried out in the entire nation. Synchronised immunisation days (SNIDs) are supplementary vaccination activities that are carried out at the same time by countries sharing common land and sea boarders. Local national immunisation days (LIDs) concerned only Provinces/Health Districts of the Nation sharing common boarders with neighbouring countries that are still declaring cases of wild poliovirus, or Provinces/Health Districts declaring cases of measles or hepatitis B or any other cases of vaccination preventable diseases. Vaccination campaigns will be used indifferently to represented them.
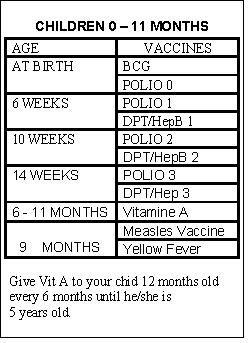
Poliomyelitis is an infectious disease caused by a virus the ‘wild poliovirus’ resulting in the paralysis of the arms or the legs. Children below 5 years are particularly vulnerable. The wild poliovirus is transmitted from an infected person to a non-infected person through the oral-faecal route. To prevent poliomyelitis each child should be completely vaccinated before the age of one year according to the national vaccination calendar of the Extended Programme on Immunisation (EPI); and should receive all the prescribed doses of polio vaccine during the national immunisation days against poliomyelitis.
National, synchronised and local immunisation days against poliomyelitis were organised in Cameroon, including the Bamenda Health District from 1996 to May 2005. The target population for National Immunisation Days against poliomyelitis is children aged 0 – 59 months. In 2002 national immunisation days against measles were effected for children 9 months to 14 years old. During some of the national immunisation days Vitamin A was administered to children 6 – 59 months. The objective of this write up is to describe the implementation process and state the results of immunisation days in Bamenda Health District from 1996 to May 2005.
GAOLS OF IMMUNISATION DAYS
1) Eradicate poliomyelitis.
2) Reduce morbidity due to measles.
3) Reduce morbidity due to Vitamin A deficiency.
OBJECTIVES OF NATIONAL IMMUNISATIONS DAYS:
1. Vaccinate all children 0 - 59 months against poliomyelitis.
2. Vaccinate all children 9 months to 14 years against measles.
3. Administer Vitamin A to all children 6 to 59 months.
4. Stop the cross-border propagation of wild polio virus through the SNIDs
5. Carry out active surveillance of acute flaccid paralysis (AFP) in children less than 15 years.
6. Educate population to adhere to the routine Expanded Programme on Immunisation.
METHOD:
Data were obtained from the following sources:a) Archives in the District Health Service
b) Reports in the office of the District Health Service
c) Archives in the Provincial Delegation of Public Health, North West
d) Reports in computer from 2001 to August 2005.
The results, sources of information of parents, some causes of refusals, and funding of some NIDs will be presented.
PREPARATORY PHASE:
a) Planning
The Central Level, the Ministry of Public Health, determines the dates and types of national immunisation days, based on results of epidemiological surveillance.
At the level of the Health District a microplan is elaborated for each national immunisation days using the national planning tool.
In Bamenda Health District each Health Area elaborates an operational one-sheet micro plan for the NID.
Members of District Health Service, Chiefs of Centres, supervisors, vaccinators, social mobilisers, and Community Members of the District Management Committee are trained.
Vaccines and materials are received and distributed.
b) Social mobilisation
Letters for social mobilization and advocacy are written to the Administrative Authorities, Traditional, Religious and Political Leaders, during each phase of the NIDs.
Community Members of the District Management Committee are trained as focal points for social mobilization.
Advocacy meetings are held before the NIDs.
Spot messages are written, recorded and broadcasted by all the radios in Bamenda; it is also used with the public announcement system of the District Health Service to mobilise the population for the vaccination campaign.
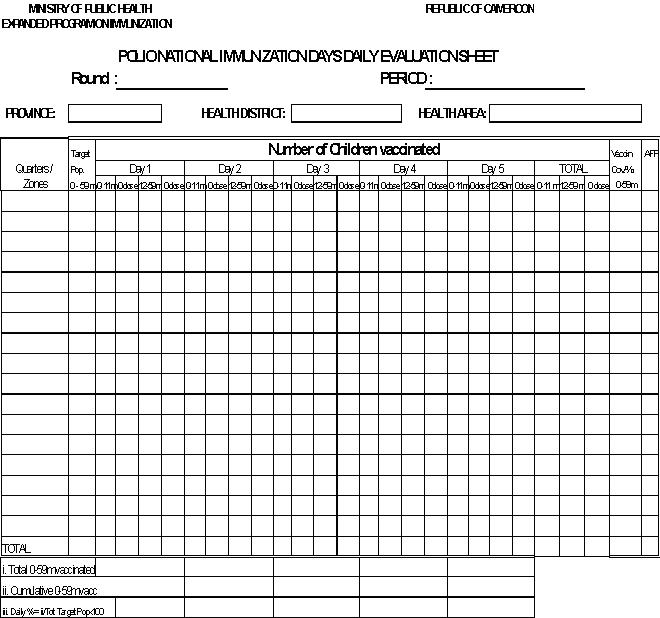
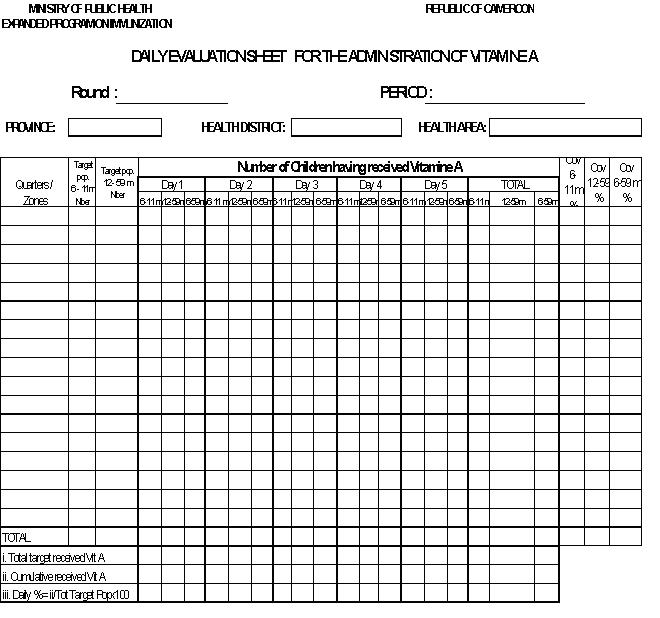
c) Tools used during NIDs
- Tally sheets
- Daily evaluation form
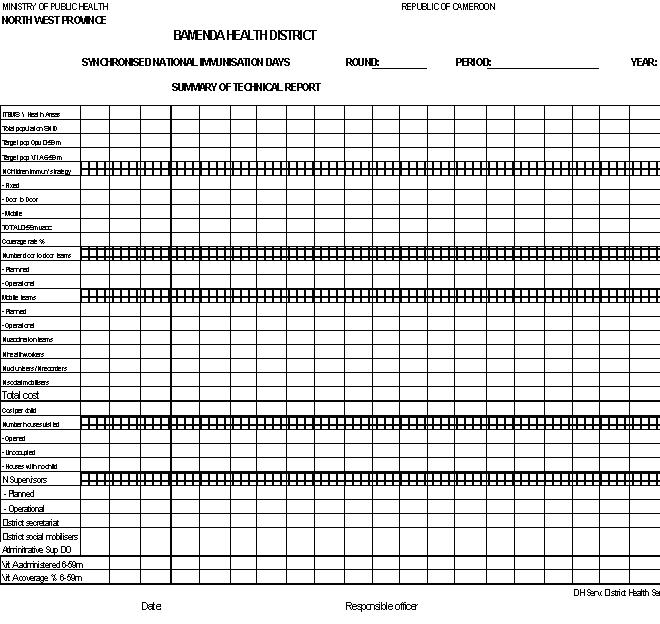
- Technical reports form
- Financial report form
- Rapid assessment questionnaire
- Form for investigation of refusals
- Form for the supervision of vaccination teams
- A sheet describing the numbering and marking of children used by each vaccination team.
This list of tools is not exhaustive.
d) Excel Computer Programmes
The author elaborated excel computer programmes for the synthesis of data collection tools used for the NIDs as from 2001, (the programmes always conformed to those from the Central Level):
- Daily evaluation form for children vaccinated, those receiving Vit A, and number of houses visited.
- Technical reports from health areas
- Financial report from health areas
- The summary form of the rapid assessment questionnaire.
IMPLEMENTATION PHASE
The local Administrative Authorities or the Minister of Public Health, or Traditional Rulers launched most of the vaccination sessions, at various levels.
The strategy for the NIDs is door-to-door for Polio; fixed and temporary sites for Measles. However the strategy for NIDs Polio evolved from fixed in 1996 to door-to-door 2000, and to door-to-door in 2001 and thereafter. Supervision is intense during NIDs with supervisors from different levels:
- Health area supervisors: responsible for the immediate supervision of vaccination teams
- District Supervisors responsible for the supervision of Chiefs of Centres and vaccination teams.
- The Provincial Supervisors responsible for the supervision of District Health Team, Chiefs of Centres and vaccination teams.
- The National Supervisor from the Ministry of Public Health
- Supervisors from either the World Health Organisation, or UNICEF
- International Consultants
Daily evaluation meetings involving the Chiefs of Centres, the District supervisors, and Community Representatives of District Management Committee, Provincial supervisors; and sometimes the National supervisors and International Consultants are held. There is a daily review of results and rapid assessment forms; positive points and weaknesses are identified and orientations for the following day adopted.
Daily Health District synthesis are made using the excel programmes, and forwarded to the Provincial Delegation of Public Health.
RESULTS OF NATIONAL IMMUNISATION DAYS
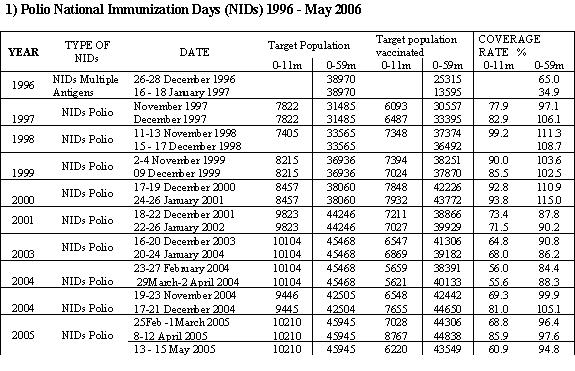
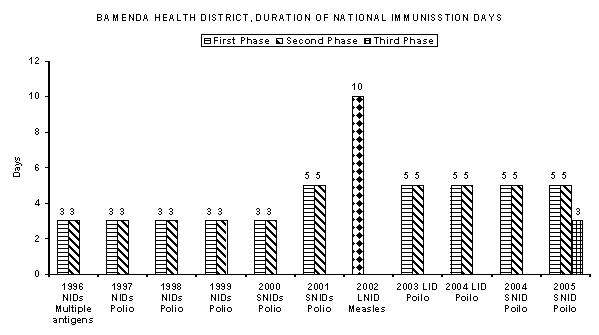
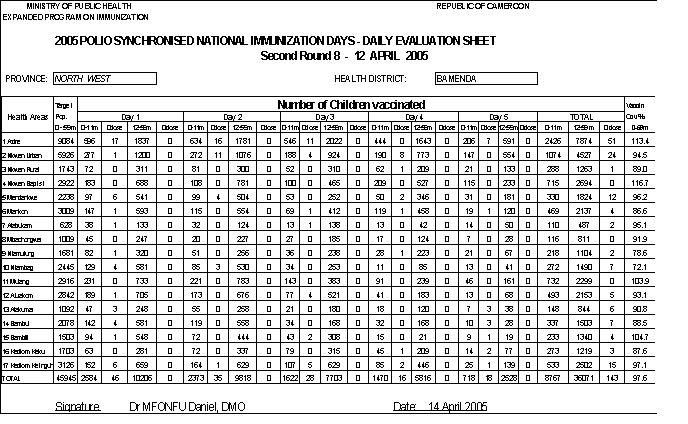
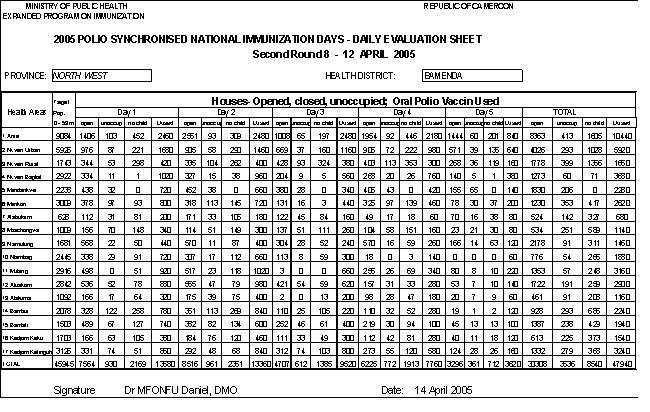
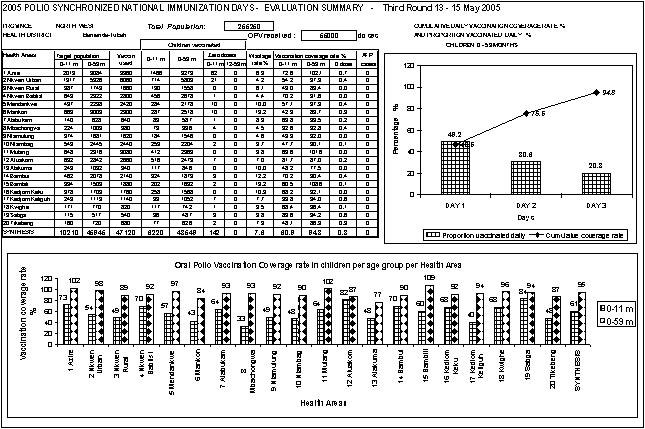
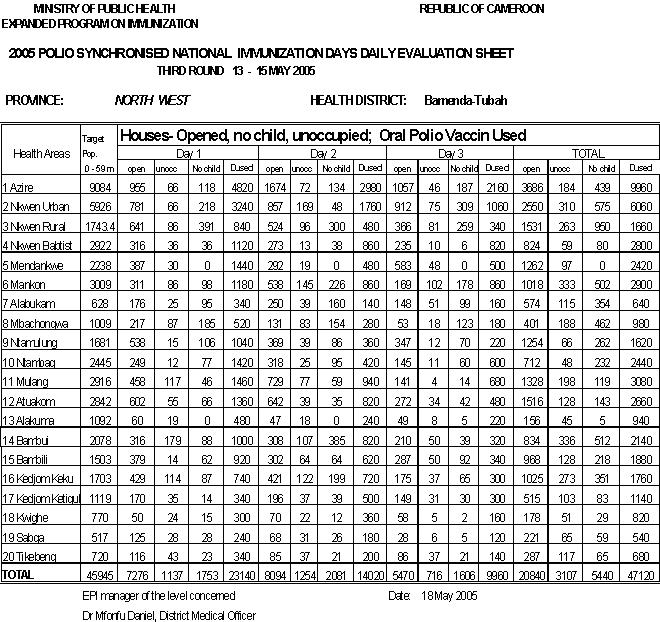
The duration of NIDs Polio varied from three days in 1996 to 2000, then five days from 2001 to April 2005, and then three days May 2005. The NIDs Measles in 2002 planned for eight days was extended to ten days because of religious feast days.
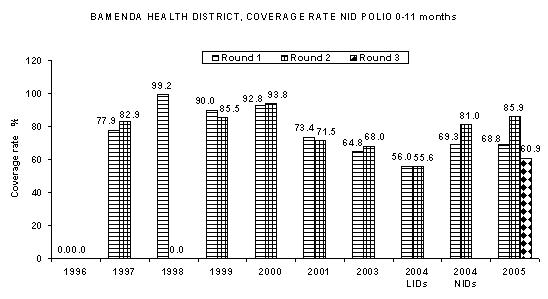
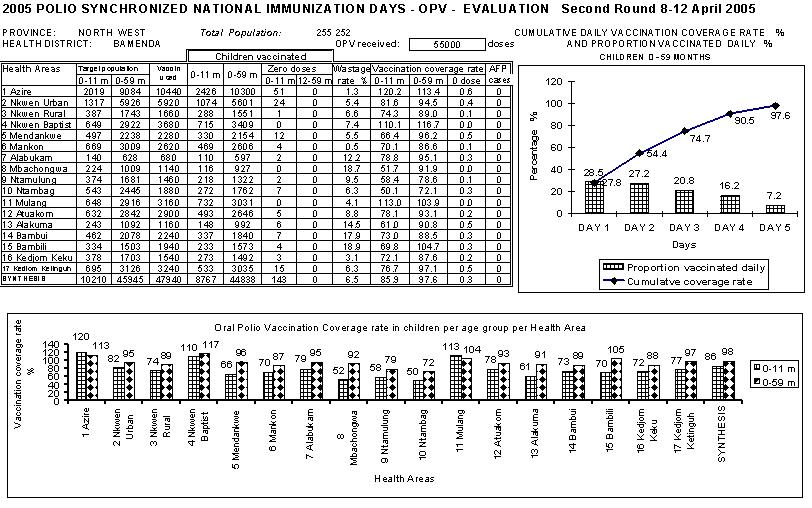
The results of vaccination campaigns for polio ranged from 65% and 34.9% in 1996 to 115.0% in 2001. Detailed results are shown in the tables and graphs below.
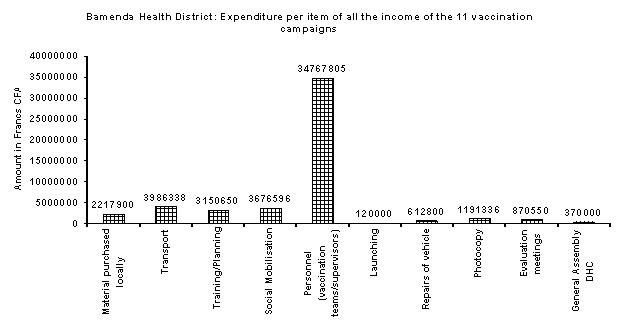
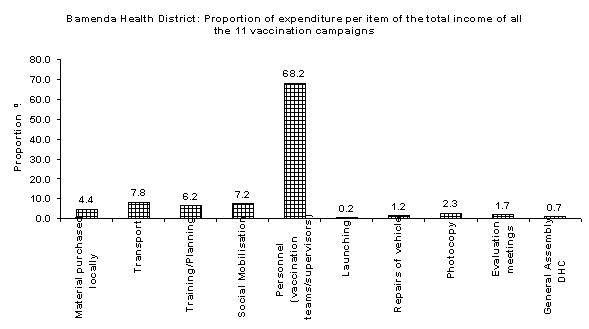
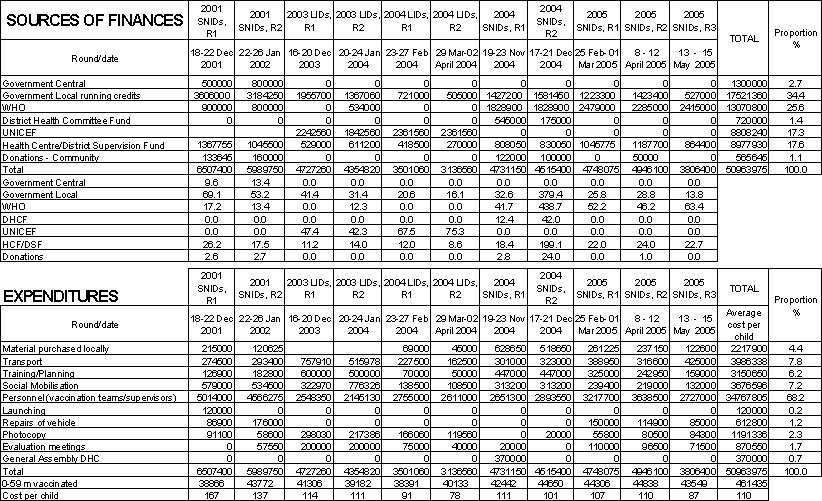
The cost of the vaccination, campaigns varied from 3136560 to 6507400 francs CFA with and average of 4633100 francs for the eleven vaccinations campaign finances considered. The average cost per child is 110 francs.
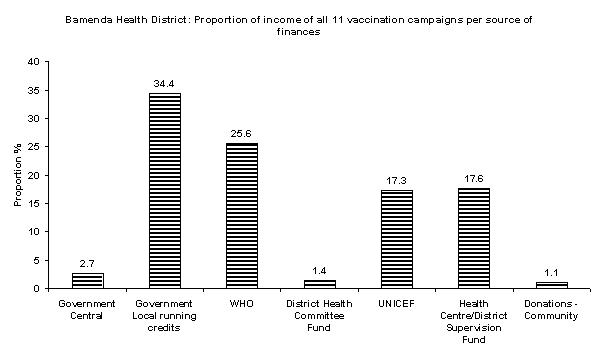
The money spent for the measles campaign of 2002 was 9442180 francs CFA with 53.0% from WHO, 36.6% from local running credits, and 10.4% from health centre funds.
The main sources of finances are the local running credits, WHO and UNICEF, local health centre funds.
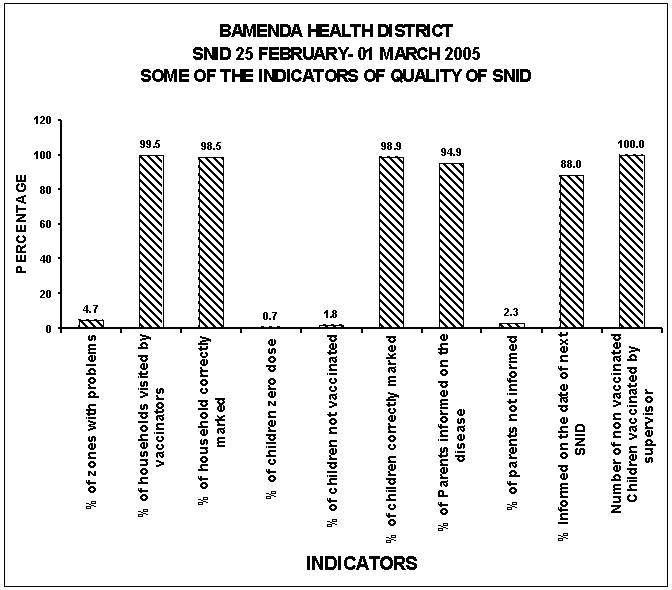
The main sources of information of parents of children as revealed by the rapid assessment were the radio 29.7%, criers and mobilisers 24.5%, churches/mosques 22.5%, and television 16.4%
The main reasons for refusals identified were children absent 47.1%, refusal by parent 17.6%, and guest child/newborn 23.5%; houses not visited 11.8% out of 17 children; all theses children were vaccinated.
All houses and stores were numbered as from the vaccination campaign of 2003; children were also systematically marked with nail polish.
1) Polio National Immunization Days (NIDs) 1996 - May 2006
View image on next POST
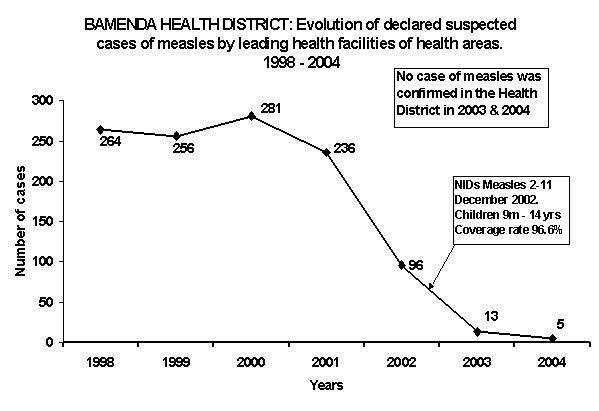
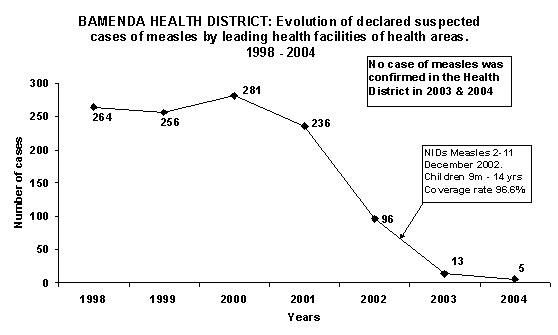
2) Measles National Immunisation Days; Monday 2 – Wednesday 11 December 2002
Target population: Children 9 months to 14 years
View image on next POST
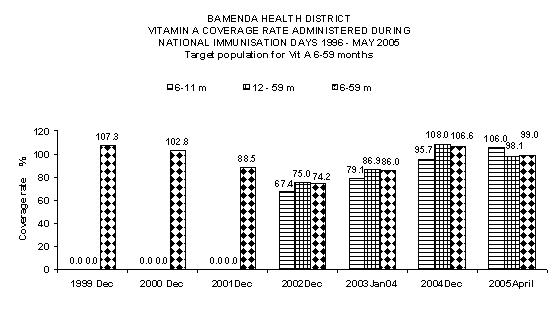
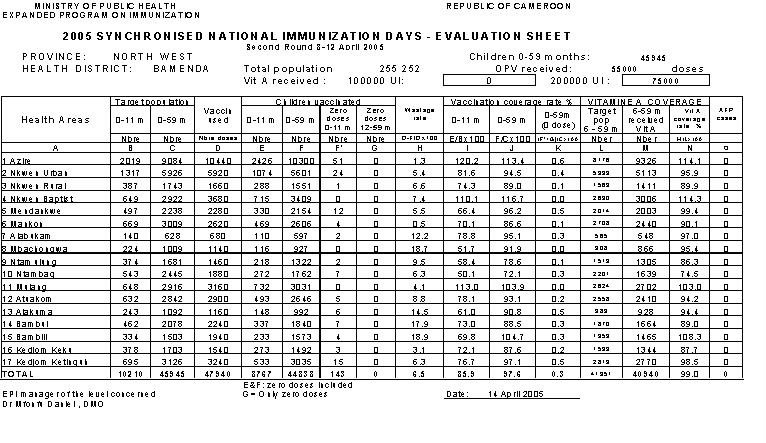
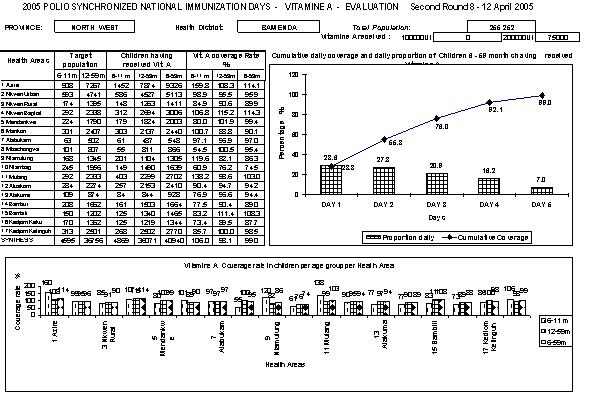
3) Vitamin A administered during National Immunization Days, 1996 – May 2005
Target population - Children 6 - 59 months
View image on next POST
DISCUSSIONS
The lowest coverage rate for Polio vaccine (65.0% and 34.9%) were obtained in 1996 because of the administration of all the vaccines of routine EPI (BCG, Polio, DPT, Measles), but after evaluation only one antigen was adopted for NIDs from 1997, sometimes with the administration of Vitamin A.
The quality of vaccination campaigns has improved over the years through the introduction evaluation tools, training of personnel, exclusive door-door-door strategy, rapid assessment, intensive supervision, numbering of houses and stores at the markets, and marking of children.
Social mobilisation is very high with the involvement of all authorities thus all refusals are vaccinated; although advocacy meetings produce very little resources. The Bamenda Urban Council and the Tubah Council offer donations.
The radios plays a very important role in social mobilisation in Bamenda, however they must be assisted by the District Health in producing a spot for broadcasting and sponsoring the cost.
A large proportion of the financing of vaccination campaigns comes from local contributions by health services through especially running credits above 34.4%.
The refusals are usually few and convinced through dialogue with the health teams at all levels including the Administrators and District focal mobilisers.
The number of children who has never received polio vaccine has greatly reduced to only few newborn of the previous night.
The active search for AFP yielded no confirmed case.
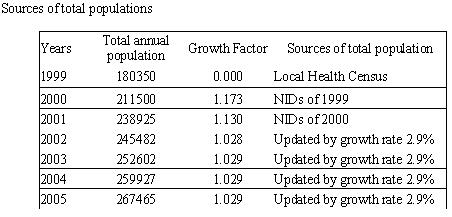
The population for the vaccination campaigns is usually updated from the highest target population vaccinated the previous year consequently there is usually no shortage of vaccine.
The radio spots conceived and produced by the author, and broadcasted over all the radio stations, although at a very high cost, plays a predominant role in social mobilisation. However sources of information varied according to health area urban/rural. The role of social mobilisers cannot be neglected.
The number of declared suspected cases of measles has greatly dropped and no case of measles has been confirmed since the NIDs against measles in 2002. The absence of measles in the community has resulted to a false impression by the population that there is no need to vaccinate children against measles again.
One always encounters inadequate finances despite the heavy use of local service finances that usually diminished according to the number vaccination campaigns during the year. There is need for aprons for all teams to facilitate recognition by the population
Communication of financing of SNID at the National level should be moderated and should include an open appeal for community participation and support of the SNID at all levels.
Social mobilisers who know their quarters very well and also well known; who participate in drawing up the itineraries and maps should constitute a member of the vaccination team even if the team is only made up of two persons.
CONCLUSION
The population has experienced the impact of vaccination campaigns for they no longer observe measles and paralysis due to poliomyelitis in the community and thereby seeing no need for vaccination. It is therefore necessary for the health personnel to intensify educate and mobilise the population to continue to vaccinate their children.
It was difficult to obtain all the results because of poor documentation system; it is therefore highly recommended that every staff should be committed to an effective filing system. Hard copies of reports in computer should be made periodically, and electronic backups should be made in order to facilitate the application the health management information system.
It is absolutely essential to elaborate simple computer excel programs for the exploitation and synthesis of all the tools used in the SNID. The author has been taking a lot of initiative in producing excel programs that enhance easy reporting. Any level can acquire this expertise in order to accomplish an excellent work.
With the enthusiasm, commitment and involvement of all the partners, community, health committee members at all levels, health personnel, the Administration and traditional rulers one should be very optimistic that Bamenda Health District will continue to play its own important role towards the eradication of wild poliovirus in Cameroon.
View image on next POST
BAMENDA HEALTH DISTRICT: FINANCING OF VACCINATION CAMPAIGNS AGAINST POLIO FROM 2001 TO MAY 2005
View image on next POST
MEASLES NATIONAL IMMUNISATION DAYS 2002
View image on next POST
SOME TOOLS DEVELOPED OR AMELIORATED TO ENHANCE PLANNING,
SYNTHESIS AND MONITORING
View image on next POST
BAMENDA HEALTH DISTRICT
SYNCHRONIZED NATIONAL IMMUNISATION DAYS (SNIDs) 2005
MARKING OF CHILDREN AND NUMBERING OF HOUSES
View image on next POST
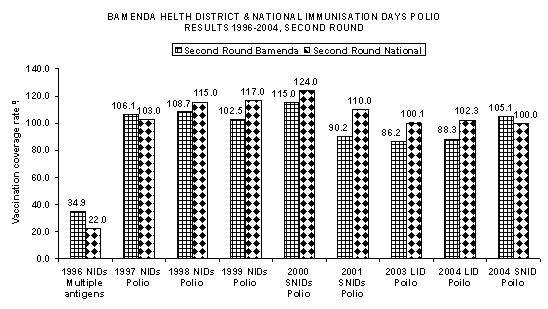
NATIONAL RESULTS OF NATIONAL IMMUNISATION DAYS (NIDs) 1996 – 2004
View image on next POST
Source: Brochure ‘Synchronised National Immunisation Days 2004 & 2005’ by Ministry of Public Health and UNICEF
NIDs: National Immunisation Days
SNIDs: Synchronised Immunisation Days
LIDs: Local Immunisation Days
View image on next POST
Sample of social mobilisation Messages
MINISTRY OF PUBLIC HEALTH REPUBLIC OF CAMEROON
------------- Peace-Work-Fatherland
PROVINCIAL DELEGATION
OF PUBLIC HEALTH
NORTH WEST PROVINCE
-------------
BAMENDA HEALTH DISTRICT
Bamenda, 17 February 2005
The District Medical Officer,
To:
The: ___________________________
Subject: Vaccination campaign against poliomyelitis. SNID POLIO 2005
‘Let us participate in the eradication of polio in Cameroon, Africa and the World’
I have the honour to inform you that poliomyelitis is still paralysing some our children, that is why the Ministry of Public Health is organising the national vaccination campaign against Polio for all children less than 5 years in our Country at the same period with Nigeria and all the countries in West and Central Africa, according to the recommendation of WHO and UNICEF.
First round from:
Friday 25, Saturday 26, Sunday 27, Monday 28, to Tuesday March 01, 2005.
Second round from:
Friday 8, Saturday 9, Sunday 10, Monday 11, to Tuesday 12
April 2005.
Vaccination teams will move from door to door and will put two drops of oral polio vaccine in the mouth of each child during the two rounds even if the child had been vaccinated.
The District Medical officer is appealing to you to use your good office to educate and mobilise your population to participate fully in these campaigns exercise.
Your usual support to the Health District Service and Health Areas will be highly appreciated.
Dr MFONFU DANIEL
DISTRICT MEDICAL OFFICER
MINISTRY OF PUBLIC HEALTH REPUBLIC OF CAMEROON
-------------. Peace-Work-Fatherland
PROVINCIAL DELEGATION
OF PUBLIC HEALTH
NORTH WEST PROVINCE
-------------
BAMENDA HEALTH DISTRICT
Bamenda 23 February 2005
No. ______ /MPH/NWP/BHD/_______
The District Medical Officer,
To;
The Chief of Station, CRTV,
Bamenda
Subject:
Subject: Synchronised National Immunisation Days against Polio (SNID) 2005
Sir,
Kindly let this cassette containing the social mobilisation spot for this SNID be played several times during this vaccination exercise. The text of the social mobilisation can be used during the news.
“The District Medical Officer,
Informs the Population of Bamenda Health District, that poliomyelitis is still paralysing some our children, that is why the Ministry of Public Health is organising the national vaccination campaign against Polio for all children less than 5 years in our Country at the same period with Nigeria and all the countries in West and Central Africa, according to the recommendation of WHO and UNICEF
The First phase will take place from:
Friday 25, Saturday 26, Sunday 27, Monday 28, February to Tuesday 01 March 2005.
The Second phase from:
Friday 8, Saturday 9, Sunday 10, Monday 11, to Tuesday 12 April 2005.
Dear parents, vaccination teams will move from door to door.
They will come to our houses, nursery schools, markets, and motor parks to vaccinate our children less than 5 years, by giving each child 2 drops of polio vaccine in mouth.
The polio vaccine is very safe. Poliomyelitis has no treatment.
Dear parents let us, as usual, have confidence in our Ministry of Public Health, WHO and UNICEF.
Let us participate in the eradication of Polio in Cameroon, Africa and the World.
Let us just present our children less than 5 years to the vaccination teams as they pass by.
Prevention is better than cure
Dr. MFONFU Daniel
District Medical Officer
Bamenda Health District
































{kind=link}